The Essex Lopresti injury is a complex series of injuries to the forearm, usually caused by fall from a height onto the outstretched hand, or a similar high energy mechanism. The injury affects 3 main structures:
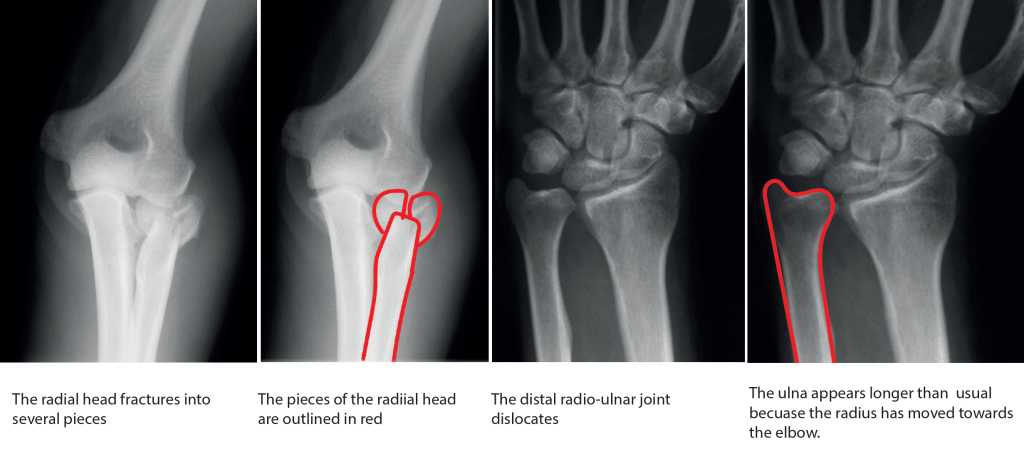
1) The radial head, which often breaks into a number of pieces.
2) The interosseous membrane – this structure is a thick piece of fibrous tissue which runs down the whole length of the forearm, connecting the forearm bones to each other.
3) The distal radio-ulnar joint, which dislocates when the entire radius bone is driven towards the elbow.

How is the injury diagnosed?
People with this injury usually have pain in their elbow primarily. This often overshadows pain in the forearm or wrist, and may focus attention on the elbow. When a broken or fractured radial head is seen on the first xray, doctors may assume that this is the only injury, and it is for this reason that this injury can be missed initially. A further xray of the wrist will show the characteristic dislocation of the distal radioulnar joint.
How is the Essex Lopresti injury treated?
Treatment of an Essex Lopresti injury needs an experienced surgeon to guide the decision making and perform the surgery, so when people with this injury present initially, it can be a frustrating few days before a plan is made, simply because surgeons with experience in treating this injury may not be available immediately.
Surgery is almost always recommended. Surgery addresses 2 of the 3 parts of this injury – The radial head is fixed with tiny screws and a plate to hold it in position during the healing process. If the radial head cannot be fixed because here are too many fragments, then a replacement radial head is inserted. The distal radioulnar joint is reduced (put back into position) and held in place with thick wires or pins which run from the ulna across the radius and these wires prevent any rotation of the forearm.
Some specialists attempt to repair or reconstruct the interosseous membrane, but this has mixed results and is not a widely used technique.

What happens after the operation?
After surgery, the forearm has to be immobilised in a long arm plaster cast, in order to protect the wires holding the distal radioulnar joint in position. This type of plaster cast is very restrictive – being unable to move your elbow makes even simple things like getting dressed very difficult. The cast is usually on for around 6 to 8 weeks, and when it comes off the wires holding the distal radioulnar joint are removed.
Getting the elbow and forearm moving again after the cast and wires are removed takes months rather than weeks. The elbow will start to bend and straighten slowly, and getting back maximum movement usually takes up to a year following the operation. Rotation of the forearm is also very restricted and takes many months to recover.
Are there exercises I should do while the cast is on?
It is really important to keep all the joints of the arm moving if they are not under the cast. Your should keep your shoulder moving as much as possible, and hand exercises should start immediately, with opening and closing the fingers as illustrated below:

How much function will return following an Essex Lopresti injury?
Everyone who has this injury reports some loss of function in the long term. Generally speaking, we expect some limitation of elbow extension, and some limitation of forearm rotation. The amount of restriction varies, but it is common to lose the last 30 degrees of elbow extension and around 50% of normal forearm rotation.
Grip strength is also affected by this injury, with most people losing around 30% of their normal grip strength because of the injury.
Are there any other complications of this injury?
Because this is a very serious injury to the forearm, there is no good way of making the arm function normally again, and coping with this loss of function can be very difficult both physically and psychologically. Many people with this injury need secondary surgery around 6-12 months after the initial injury in order to maximise function:
1) Removal of the fixation plate and screws from the elbow is commonly recommended because these tend to actively restrict movement. Taking the metal out, however, never restores full movement, because of the scar tissue that surrounds the bones.
2) Where a radial head replacement has been used, this can produce signifiant pain at the elbow caused by the forces crossing the metal onto the bone of the humerus. The replacement radial head sometimes has to be removed.
3) Some people have long term ‘instability’ of the forearm, with further operations needed both at the elbow and at the wrist to try and prevent impingement of the bones.

© Fife Hand Service 2023
